
About FGM/C
Female Genital Mutilation (FGM) is also known as Female Genital Cutting (FGC) or Female Circumcision. It is traditionally practiced in many ethnic groups all over the world. While Africa, Asia, Australia and other continents have documented FGM/C, gradually FGM is being recorded in places where migrants from the practicing communities settle. Worldwide, the exact number of girls and women who have undergone FGM/C remains unknown. However, at least 200 million girls and women in 30 countries, mostly in Africa, have been subjected to the practice. Furthermore, globally it is estimated that 3 million girls are at risk of undergoing female genital mutilation every year. Even though the ages for FGM/C vary between communities, the majority of girls are cut before they turn 15 years old. In other places, baby girls under the age of five are victims of the practice. Eliminating FGM/C by 2030 is one of the Sustainable Development Goals, which are 17 global goals set by the United Nations in 2015.
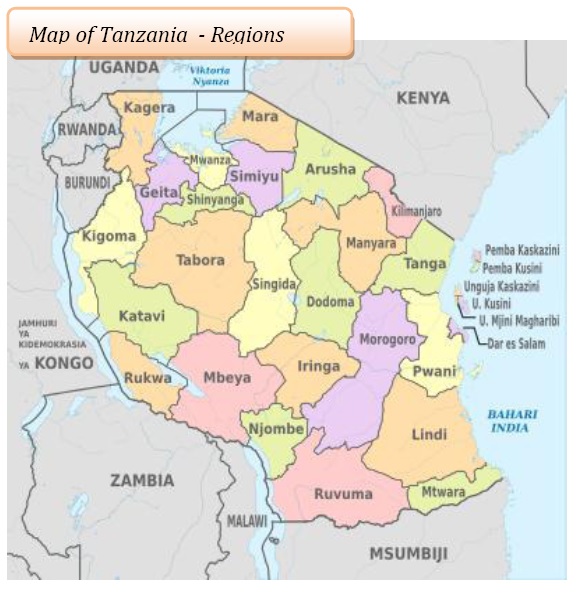
Tanzania is one of many countries in Africa whose ethnic groups practice FGM/C. There are over 120 different ethnic groups living in 30 administrative regions. FGM/C is practiced in 25 of these regions of which 12 have a prevalence rate of between 4.2 to 57.7%. The Manyara region in the northern zone has the highest rate of FGM (57.7%) in the country, followed by Arusha (41.0%), Tanga (13.7%) and Kilimanjaro (10.1%). The central zone which includes Dodoma (46.7%), Singida (30.9%) and Tabora (0.6%) has the average highest FGM/C prevalence rate of 45.6% according to the Tanzania Demographic Health Survey 2015/2016. Please see the link below for more information:
http://www.nbs.go.tz/nbstz/index.php/english/statistics-by-subject/health-statistics/demographic-and-heal
FGM/C is against human rights and a criminal offence under the law in Tanzania as defined in the Sexual Offences Special Provision Act of 1998 - penal code 169A and in the Law of the Child Act of 2009, article 13 (1). The FGM/C awareness is estimated at above 80% in Tanzania. However, the practice is still prevalent with an average of 10%. However, in the practicing communities the rates may be as high as 100%.
The FGM/C
Female Genital Mutilation (FGM), also referred to as “Female Genital Cutting (FGC),” has been defined by the World Health Organization (WHO) as “all procedures involving partial or total removal of the external female genitalia or other injury to the female genital organs for non-medical reasons” (WHO 2008). Once characterized as “female circumcision,” the word “mutilation” was adopted both to distinguish it from male circumcision and to stress the severity of the act (WHO, UNICEF, UNFPA 1997). A hybrid term – “female genital mutilation/cutting” – was coined by the UNFPA-UNICEF Joint Programme to underscore the importance of using non-judgmental terminology with practicing communities while emphasizing the fact the female genital mutilation/cutting constitutes a violation of the human rights of women and girls.
Classification of FGM/C
The UN Interagency group (WHO, UNICEF and UNFPA) classify FGM/C in four types which are:-
- Type I: Clitoridectomy: partial or total removal of the clitoris (a small, sensitive and erectile part of the female genitals) and, in very rare cases, only the prepuce - the fold of skin surrounding the clitoris.
- Type 2: Excision: partial or total removal of the clitoris and the labia minora, with or without excision of the labia majora (the labia are "the lips" that surround the vagina).
- Type 3: Infibulation: narrowing of the vaginal opening through the creation of a covering seal. The seal is formed by cutting and repositioning the inner, or outer, labia, with or without removal of the clitoris.
- Type 4: Other: all other harmful procedures to the female genitalia for non-medical purposes e g pricking piercing incising scraping and cauterizing the medical purposes, e.g. pricking, piercing, incising, scraping and cauterizing the genital area
FGM/C procedure
The practicing communities in Tanzania use elderly women to carry out the procedure. They are popularly known as ‘Ng’ariba’ or female circumcisers who pass on the skills to other female members of their families. The circumcisers are socially accepted, feared, respected and fulfill multiple socio-cultural roles. In many cases, circumcisers are also traditional midwives.
Home made knives, razor blades, broken glass, tin-lids, scissors and other sharp objects are used to cut multiple girls depending on the number, which is pre-determined. Early in the morning, prior to the procedure, girls are required to bath in cold water which is believed to lessen the pain since no anaethesia is used. Usually, the procedure happens in temporary tents made of local materials in bushes near their homes. Generally, the environment and tools are unclean with a high contamination risk. To avoid excessive blood loss the circumcisers apply crushed dry leaves, ash from certain trees and others use raw eggs. FGM/C is also reported to happen in health institutions perpetrated by some medical practitioners.
FGM/C is mostly carried out on girls between the ages of 0 and 15 years. However, occasionally, adult and married women are also subjected to the procedure. The age at which FGM/C is performed varies with local traditions and circumstances.
International and regional instruments against FGM/C
There is strong support for the protection of the rights of women and girls in abandoning FGM/C in international and regional human rights treaties and consensus documents which are not limited to:-
- International treaties
- Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment
- Covenant on Civil and Political Rights
- Covenant on Economic, Social and Cultural Rights
- Convention on the Elimination of all Forms of Discrimination against Women (CEDAW)
- Convention on the Rights of the Child
- Convention relating to the Status of Refugees and its Protocol relating to the Status of Refugees
- Regional treaties
- African Charter on Human and Peoples’ Rights (the Banjul Charter) and its Protocol on the Rights of Women in Africa - Maputo Protocol.
- African Charter on the Rights and Welfare of the Child
- European Convention for the Protection of Human Rights and Fundamental Freedoms
- Consensus documents
- Beijing Declaration and Platform for Action of the Fourth World Conference on Women
- General Assembly Declaration on the Elimination of Violence against Women
- Programme of Action of the International Conference on Population and Development (ICPD)
- UNESCO Universal Declaration on Cultural Diversity
- United Nations Economic and Social Council (ECOSOC), Commission on the Status of Women. Resolution on Ending Female Genital Mutilation.
Effects from FGM/C
FGM/C has a number of physical, psychosocial, medical and economical effects. The immediate effects include severe pain, swelling on the genitals, loss of blood, fractured bones or dislocations, HIV/AIDS infection and death. Victims also often suffer from nightmares, anger, urinary tract infections and an infected wound.
Long term effects include:-
- Pain: due to tissue damage and scarring that may result in trapped or unprotected nerve endings.
- Infections: (chronic genital infections, chronic reproductive tract infections and urinary tract infections)
- Painful urination: due to obstruction of the urethra and recurrent urinary tract infections.
- Menstrual problems
- Keloids
- Human immunodeficiency virus (HIV)
- Female sexual health – painful sexual intercourse.
- Obstetric complications – difficult deliveries and obstetric tears/lacerations
- Obstetric fistula
- Perinatal risks due to obstetric complications may lead into high incidence of infant resuscitation at delivery and intrapartum stillbirth and neonatal death
- Psychological consequences - Post-Traumatic Stress Disorder (PTSD), anxiety disorders and depression
Reasons for the FGM/C practice
FGM/C is practiced for a number of reasons including cultural, religious and social beliefs which are maintained and preserved by older generations. Grandparents, parents and close relatives ensure the practice is upheld to maintain family and community status. Peer pressure from men, women and children forces the victims to succumb to the their families' demands. Moreover, the low socio-economic status of women together with the lack of formal education also increases the likelihood of the practice.
Women and girls are made to believe that FGM/C should happen because it is seen as a rite of passage from childhood to adulthood. They believe it makes women clear, strong and beautiful. Girls who undergo FGM/C have a better chances in the marriage market and are associated with higher bride prices compared to those who refuse to undergo FGM/C. Rituals within families and in their communities are conducted by women who have themselves undergone FGM/C which entitles them to a degree of respect among the community.
Ending FGM/C
FGM/C is a cultural practice which has been in existence for generations. It is linked to the belief that women's sexual desire needs to be controlled and it is also has a socio-cultural identity. The practice goes against basic human rights and is criminalized by the law in Tanzania. NAFGEM realizes that the continuation of the practice is due to a number of factors including conservative traditionalistic societies, ignorance of the anatomy and physiology of the female reproductive organs, a lack of awareness of fundamental human rights and the law, inadequate protection and social services available to the practicing communities and the poor socio-economic status of women and girls among these communities. Furthermore, the secrecy surrounding the practice creates a big challenge in obtaining information which would otherwise have been used to inform new interventions and projects to end FGM/C.
Ending FGM/C requires multiple approaches which will contribute towards community awareness and influence socio-cultural transformation. So far, NAFGEM implements public awareness campaigns which target different social groups including men, women, youths, children, local leaders and other collaborators, provides safe shelter services, promotes girls' education, provides livelihood skills to women and girls; and also networks with likeminded partners. Other interventions include intergenerational dialogues to break the silence, the application of the law and providing psychosocial support to victims.